
Structure of the Hip
The femoroacetabular joint, the hip joint, is a ball and socket joint that joins the femur to the pelvis. The ball corresponds to the head of the femur and the socket corresponds to the acetabulum. This ball and socket articulation allows for a high degree of stability. The femoral head and acetabulum are lined with a thin layer of smooth articular cartilage that cushions and protects the bones, preventing them from rubbing against each other. Lining the hip socket is a special ridge of cartilage referred to as the labrum that helps secure the femoral head in place.
What is FAI?
Femoroacetabular impingement (FAI), also known as hip impingement, is described as a structural and mechanical disorder of the hip. It can occur in all age groups, but it is especially common in young athletes. Impingement occurs when something prevents the normal range of motion of this ball and socket joint. Symptoms of FAI usually arise when the bones of your hip joint come too close and pinch tissue or cause too much friction. The pinching and rubbing occurs when the head and neck of the femur make contact with the acetabulum. This is mainly due to abnormal bone overgrowth on either the surface of the femoral head/neck or on the surrounding surface of the acetabulum; in most cases, this occurs during childhood development. Eventually, FAI causes damage to the labrum and/or to the articular cartilage which have poor healing capacity.
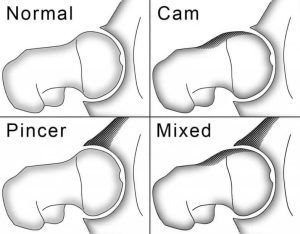
There are three types of FAI:
- Pincer type: this type of impingement occurs because extra bone extends out over the normal rim of the acetabulum, excessively covering the socket relative to the femoral head causing the labrum to be crushed under the prominent rim. Seen more in female athletes in their 30s and 40s.
- Cam type: with cam impingement the femoral head is not perfectly round mostly due to a bony outgrowth which impedes it from rotating smoothly inside the acetabulum. Seen more in male athletes in their 20s.
- Combined type: meaning that both, pincer and cam types, are present.
Many patients may have radiographic evidence of FAI and develop no symptoms at all throughout their long, active lives. When symptoms do develop it is usually indicative that damage to the surrounding cartilage or labrum has been done and that it is likely to progress. Who’s at risk? – FAI is common in high performance athletes who have the tendency to overwork the hip joint more than the average person, because of this, athletes may develop symptoms much earlier than those patients who are less active.
Symptoms and Clinical Findings
Many patients with FAI may be asymptomatic their whole lives. Symptoms of FAI may overlap with other causes of hip pain such as hip flexor tendinitis, lumbar spine radiculopathy, or testicular pain. Those that do develop symptoms may experience but are not limited to the following:
- Pain or achiness at the inner hip or groin area, usually after walking or prolonged sitting.
- Locking, clicking, or catching sensation of the joint.
- Pain while sitting for prolonged periods.
- Difficulty putting on shoes.
- Difficulty walking on slanted surfaces (i.e. up a hill).
- Pain at the lower back, buttocks, or side of the hip.
When evaluating the source of hip pain, the physician may perform a combination of provocative tests and radiographic imaging to make the diagnosis of FAI. As part of the physical exam, the doctor will assess the character of the hip pain based on patient history, the hip’s range of motion and take notice on the positions that illicit pain or discomfort. An impingement test, where the physician brings the knee up towards the chest and then rotates it inward toward the opposite shoulder, may illicit pain and if so the test is positive for impingement.
Besides physical findings, the doctor may confirm his suspicion with radiographic imaging such as X-rays, CT scans, and MRI. X-rays provide good details of bone surfaces and may show if a patient’s hip has abnormal shapes consistent with FAI. CT scans are a bit more sophisticated than X-rays and may provide better details about the dimensions of the bones. MRI are more specific to soft tissues like cartilage and labral tissue, therefore, it can provide details on the amount of damage these tissues have suffered due to hip impingement. Other diagnostic tests that may localize the source of pain are by applying local anesthetic into the joint itself. If the numbing medication provides temporary pain relief, it confirms the diagnosis.
Treatment and Outcome
Hip impingement is caused by a bony abnormality of the joint, the abnormal bone shape does not cause pain. However, other structures that become injured such as the labrum or articular cartilage may be responsible for the pain experienced by patients with FAI. When symptoms are mild and pain is manageable, physicians will always prefer nonsurgical treatment options, but when symptoms are persistent and severe, surgical options may be considered. When left untreated, FAI may lead to degenerative changes and osteoarthritis of the hip in the long-term.
Initially, when symptoms develop, it is beneficial for the patient to try and identify activities or movements that cause pain. Modifying such activities and allowing the hip joint to rest may resolve the initial pain symptoms. If activity modification and rest is not suffice, then medication therapy with NSAIDs, such as ibuprofen, may reduce pain and inflammation. Physical therapy may also be considered, which can improve range of motion and strengthen muscles that support the joint. This may relieve stress on the injured labrum or cartilage.
When evidence of joint damage is present and pain cannot be relieved with conservative therapy, the physician may recommend surgery. Most FAI problems can be treated with arthroscopic surgery. Arthroscopy is done by making small incisions around the joint and then introducing thin instruments – a small camera and a shaver – to visualize and repair the damaged tissue. Once inside the hip joint, besides repairing the damaged labrum and/or cartilage, the surgeon is also able to trim down the bony deformities either on the rim of the acetabulum or the fermoral head to improve movement of the joint. Surgical correction of FAI may help prevent future damage to the hip joint. The ability of surgery to successfully resolve the symptoms caused by impingement greatly depend on the severity of the damage in the first place. And although there is a small chance that surgery may not help, it is currently the best way to treat painful FAI.
Author Ernesto P. Quinones Gonzalez MS3 Third year Medical Student at University of Medicine and Health Sciences (UMHS)